Effect of low dose acetylsalicylic acid and anticoagulant on clinical outcomes in COVID‐19, analytical cross‐sectional study
Muhammad B Malik, Samar A Amer, Eric Merrell, Ronald Russo, Jeffrey B Riley, Austin Scro, Elizabeth James, Anderson Anuforo, Soumya Adhikari, Rosalie Siciliano, Philip Chebaya, Edward Darling, Michael Kuhn, Gary Nieman, Ahmed Shawkat, Hani Aiash
Health Science Reports, doi:10.1002/hsr2.699
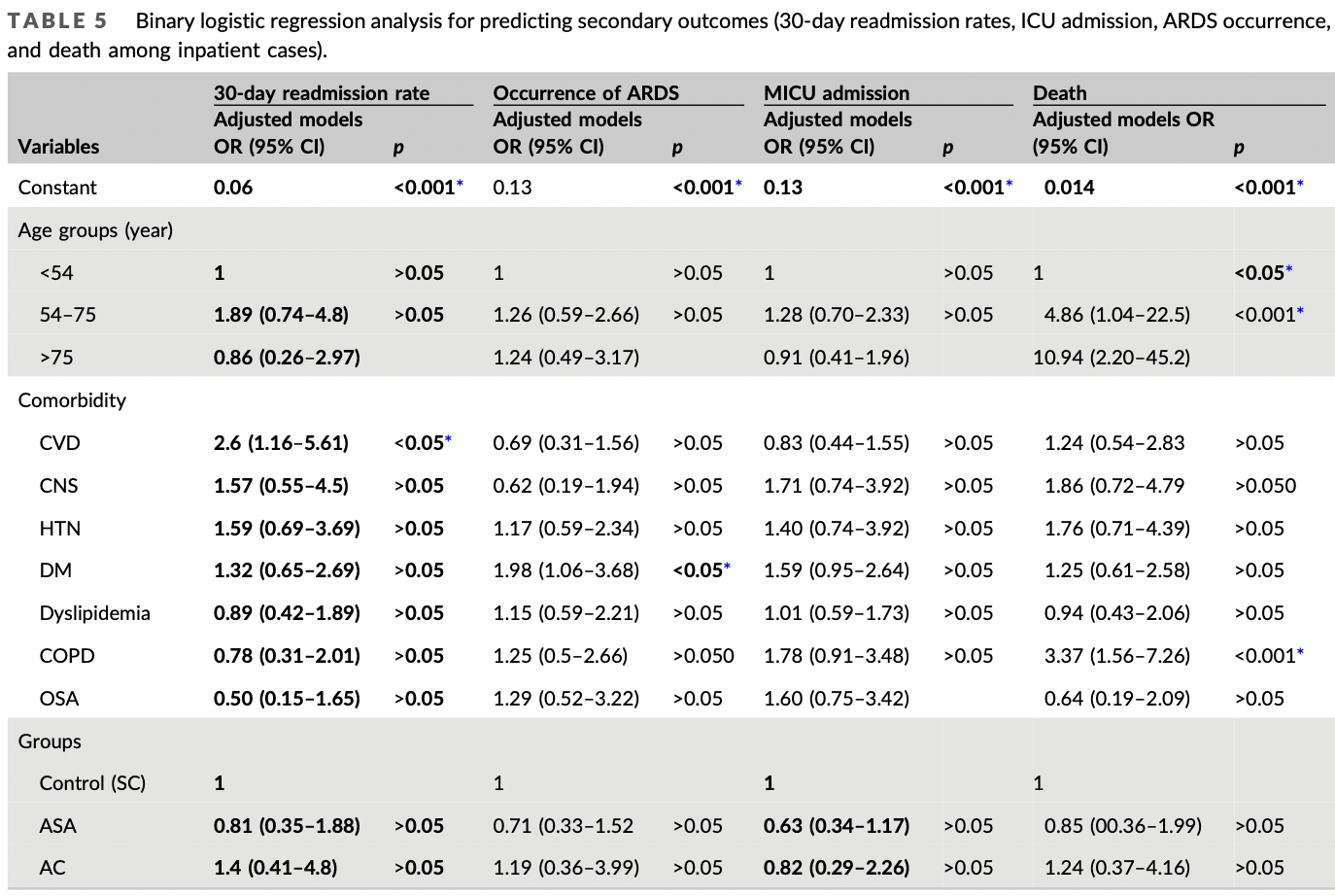
Background and aims: The therapeutic strategy for the treatment of known sequelae of COVID-19 has shifted from reactive to preventative. In this study, we aim to evaluate the effects of acetylsalicylic acid (ASA), and anticoagulants on COVID-19 related morbidity and mortality. Methods: This record-based analytical cross-sectional study targeted 539 COVID-19 patients in a single United States medical center between March and December 2020. Through a random stratified sample, we recruited outpatient (n = 206) and inpatient (n = 333) cases from three management protocols, including standard care (SC) (n = 399), low-dose ASA only (ASA) (n = 112), and anticoagulation only (AC) (n = 28). Collected data included demographics, comorbidities, and clinical outcomes. The primary outcome measure was inpatient admission. Exploratory secondary outcome measures included length of stay, 30-day readmission rates, medical intensive care unit (MICU) admission, need for mechanical ventilation, the occurrence of acute respiratory distress syndrome (ARDS), bleeding events, clotting events, and mortality. The collected data were coded and analyzed using standard tests. Results: Age, mean number of comorbidities, and all individual comorbidities except for asthma, and malignancy were significantly lower in the SC compared to ASA and AC. After adjusting for age and comorbidity via binary logistic regression models, no statistical differences were found between groups for the studied outcomes. When compared to the SC group, ASA had lower 30-day readmission rates (odds ration
from March until December, and the many outcomes were studied in detail. Every case fulfilling the selection criteria has an equal chance of being recruited into the sample (so it is a random sample) to find the association and risk assessment.
| CONCLUSIONS Low-dose ASA is a promising, effective, protective medication in potentially improving the outcomes in COVID-19 cases, through reducing mortality, and morbidity (hospital readmission rates, the occurrence of ARDS, and ICU admission) but not statistically significant due to the higher risk patients in these groups. further prospective research is still needed.
| RECOMMENDATION
CONFLICT OF INTEREST The authors declare no conflict of interest.
TRANSPARENCY STATEMENT I affirm that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
ETHICS STATEMENT This study was reviewed by the institutional review board (IRB) at Upstate Medical University and was considered exempt according to the #4(iii) exemption category in federal regulations. The requirement for written informed consent was waived by the IRB and the study was conducted in accordance with ethical principles.
References
Aghajani, Moradi, Amini, Decreased in-hospital mortality associated with aspirin administration in hospitalized patients due to severe COVID-19, J Med Virol,
doi:10.1002/jmv.27053Ahmed, Merrell, Ismail, Rationales and uncertainties for aspirin use in COVID-19: a narrative review, Family Med Commun Health,
doi:10.1136/fmch-2020-000741Chow, Khanna, Kethireddy, Aspirin use is associated with decreased mechanical ventilation, intensive care unit admission, and in-hospital mortality in hospitalized patients with coronavirus disease 2019, Anesth Analg,
doi:10.1213/ANE.0000000000005292Formiga, Rubio-Rivas, Mora-Luján, Does admission acetylsalicylic acid uptake in hospitalized COVID-19 patients have a protective role? Data from the spanish SEMI-COVID-19 registry, Intern Emerg Med,
doi:10.1007/s11739-021-02870-1Glatthaar-Saalmüller, Mair, Saalmüller, Antiviral activity of aspirin against RNA viruses of the respiratory tract-an in vitro study, Influenza Other Respir Viruses,
doi:10.1111/irv.12421Griffin, Jensen, Khan, Arterial thromboembolic complications in COVID-19 in low-risk patients despite prophylaxis, Br J Haematol,
doi:10.1111/bjh.16792Liu, Huang, Li, Effect of low-dose aspirin on mortality and viral duration of the hospitalized adults with COVID-19, Medicine,
doi:10.1097/MD.0000000000024544Martha, Pranata, Lim, Wibowo, Akbar, Active prescription of low-dose aspirin during or prior to hospitalization and mortality in COVID-19: a systematic review and meta-analysis of adjusted effect estimates, Int J Infect Dis,
doi:10.1016/j.ijid.2021.05.016Mazloomzadeh, Khaleghparast, Ghadrdoost, Effect of intermediate-dose vs standard-dose prophylactic anticoagulation on thrombotic events, extracorporeal membrane oxygenation treatment, or mortality among patients with COVID-19 admitted tothe intensive care unit, JAMA,
doi:10.1001/jama.2021.4152Merzon, Green, Vinker, The use of aspirin for primary prevention of cardiovascular disease is associated with a lower likelihood of COVID-19 infection, FEBS J,
doi:10.1111/febs.15784Pranata, Huang, Lim, Wahjoepramono, July, Impact of cerebrovascular and cardiovascular diseases on mortality and severity of COVID-19-systematic review, meta-analysis, and meta-regression, J Stroke Cerebrovasc Dis,
doi:10.1016/j.jstrokecerebrovasdis.2020.104949Samar, Albeladi, Elshabrawy, Role of neutrophil to lymphocyte ratio as a prognostic indicator for COVID-19, Health Sci Rep,
doi:10.1002/hsr2.442Wang, Li, Gu, Wang, Liu et al., Effect of antiplatelet therapy on acute respiratory distress syndrome and mortality in critically ill patients: a meta-analysis, PLoS One,
doi:10.1371/journal.pone.0154754Wen, Hsiao, Chan, Lin, Shen et al., Acute respiratory infection and use of nonsteroidal anti-Inflammatory drugs on risk of acute myocardial infarction: a nationwide casecrossover study, J Infect Dis,
doi:10.1093/infdis/jiw603Yuan, Chen, Li, Chen, Wang et al., Mortality and prehospitalization use of low-dose aspirin in COVID-19 patients with coronary artery disease, J Cell Mol Med,
doi:10.1111/jcmm.16198


{kind=link}
{kind=link}